The Old Hippie, that way of "getting around it" , the cells being replaced, rather supports the conventional idea of a soul does it not ?
Or are you just a clone of the not so old hippie of 7 years ago ?
by NAVYTOWN 29 Replies latest jw friends

The Old Hippie, that way of "getting around it" , the cells being replaced, rather supports the conventional idea of a soul does it not ?
Or are you just a clone of the not so old hippie of 7 years ago ?
Too many people come back from being clinically dead that heard everything and saw everything going on.
Then they weren't dead were they!
Then they weren't dead were they
No you're right they weren't. That's why they're called Near Death Experiences. They've experiencing something incredible that apparently happens when you're near death. And no, all of these experiences cannot simply be dismissed as 'hallucinations' or 'lucky guesses'. Two of the best cases that have been studied is the Pam Reynolds Case and the 'Denture Man Case'.
I can't seem to link them, but if you're interested, here they are: http://www.near-death.com/experiences/evidence01.html
I have a computer. What makes my computer unique and different from anyone else's is the information that I save, i.e., programs, mp3's, pictures, etc. One day my computer will wear out, just like all material things do. But, the information that I have saved can live on. I can take the hard drive (brain) out and put it in another computer (body). Or, I can transfer the information, wirelessly, into another computer!
I believe that anyone reading this gets the idea that I am making. The important thing is the DATA (soul), NOT the computer (body). Now, I personally DO NOT believe in much of anything that the Watchtower teaches, and to be honest, I don't put a lot of stock into the Bible. Nevertheless, I most definitely DO believe in a higher source that created the earth and mankind. If man has devised a way to transfer information, wirelessly, into other objects, who's to say that a higher source cannot transfer the soul (information) into another body, whether it is a physical body or a spiritual body?
I don't know and I am not saying that what I have put forth is fact, I just throw it out there as a possibility.
Lets take the Pam Reynolds case ......"Pam" was a woman who during brain surgery for a cerebral aneurysm experienced some complications. According to the account the EEG readings of her cortex and brainstem had flatlined. After the op she described a detailed near death experience (NDE), Including an out of body experience (OBE). Her descriptions were verified by medical staff in attendance at the operation. Sounds convincing but not beyond scrutiny or rebuttal as the following shows.......
http://infidels.org/library/modern/keith_augustine/HNDEs.html
As Michael Sabom recounts in Light and Death, in August 1991 a then 35-year-old woman he called "Pam Reynolds" (a pseudonym) underwent an innovative procedure to remove a brain aneurysm. The procedure—inducing hypothermic cardiac arrest or "standstill"—involved lowering Pam's body temperature to 60°F, stopping her heart and breathing, and draining the blood from her brain to cool it and then reintroduce it. When her body temperature had reached 60°F and she had no electrical activity in her brain, her aneurysm was removed. About 2 hours after awaking from general anesthesia, Pam was moved into the recovery room still intubated (Sabom, "Light" 46-47). At some point after that, the tube was removed from her trachea and she was able to speak. She reported a classic NDE with a vivid OBE, moving through a "tunnel vortex" toward a "pinpoint of light" that continually grew larger, hearing her deceased grandmother's voice, encountering figures in a bright light, encountering deceased relatives who gave her "something sparkly" to eat, and being 'returned' to her body by her deceased uncle (Sabom, "Light" 42-46).
The case was quickly celebrated because of the lack of synaptic activity within the procedure and Pam's report of an apparently veridical OBE at some point during the operation. But it has been sensationalized at the expense of the facts, facts which have been continually misrepresented by some parapsychologists and near-death researchers.[14] Although hailed by some as "the most compelling case to date of veridical perception during an NDE" (Corcoran, Holden, and James), and "the single best instance we now have in the literature on NDEs to confound the skeptics" (Ring, "Religious Wars" 218), it is in fact best understood in terms of normal perception operating during an entirely nonthreatening physiological state.
Two mischaracterizations of this case are particularly noteworthy, as their errors of fact greatly exaggerate the force of this NDE as evidence for survival after death.[15] First, in their write-up of the first prospective study of NDEs, van Lommel and colleagues write:
Sabom mentions a young American woman who had complications during brain surgery for a cerebral aneurysm. The EEG [electroencephalogram] of her cortex and brainstem had become totally flat. After the operation, which was eventually successful, this patient proved to have had a very deep NDE, including an out-of-body experience, with subsequently verified observations during the period of the flat EEG [emphasis mine] (van Lommel et al. 2044).
Second, in his Immortal Remains—an assessment of the evidence for survival of bodily death—Stephen Braude erroneously describes the case as follows:
Sabom reports the case of a woman who, for about an hour, had all the blood drained from her head and her body temperature lowered to 60 degrees. During that time her heartbeat and breathing stopped, and she had both a flat EEG and absence of auditory evoked potentials from her brainstem.... Apparently during this period she had a detailed veridical near-death OBE [emphasis mine] (Braude 274).
But anyone who gives Sabom's chapters on the case more than a cursory look will see two glaring errors in the descriptions above. First, it is quite clear that Pam did not have her NDE during any period of flat EEG.[16] Indeed, she was as far as a patient undergoing her operation could possibly be from clinical death when her OBE began.[17] Second, she had no cerebral cortical activity for no longer than roughly half an hour. Both of these facts are nicely illustrated in Figure 1 below.
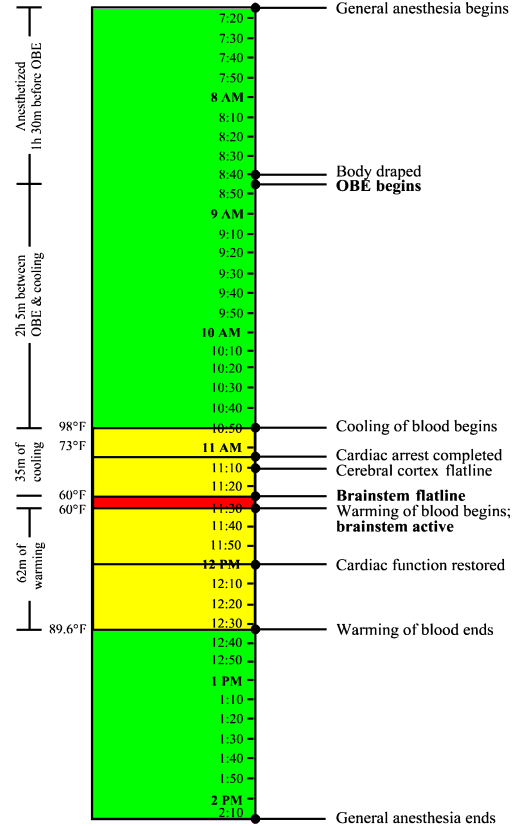
Fig. 1. Timeline of Pam Reynolds' general anesthesia. The colored areas represent changes in body temperature: Green indicates a life-sustaining temperature; yellow, the mechanical cooling or warming of blood; red, the constant temperature of her deepest hypothermia. Most times marking events or temperatures are derived from Michael Sabom's account of Pam Reynolds' procedure provided in Chapters 3 & 10 of Light & Death.
Despite accurately reporting the facts, Sabom himself has encouraged these misrepresentations.[18]Though he informs the reader that Pam's experience began well before standstill, he reveals this incidentally, so that a careful reading of the text is required to discern the point. For instance, just after describing Pam's recollections of an operating room conversation, he notes, almost as an afterthought, that "[h]ypothermic cardiac arrest would definitely be needed" [emphasis mine] (Sabom, "Light" 42). He then goes on to assert that the very features of her experience which cannot be timed happened duringstandstill. At first, Sabom only implies this by describing the cooling of blood leading to standstill prior todescribing the remainder of Pam's near-death experience (42-46). Then Sabom turns to a discussion of whether Pam was "really" dead during a portion of her standstill state:
But during "standstill," Pam's brain was found "dead" by all three clinical tests—her electroencephalogram was silent, her brain-stem response was absent, and no blood flowed through her brain. Interestingly, while in this state, she encountered the "deepest" near-death experience of all Atlanta Study participants....
With this information, can we now scientifically assert that Pam was either dead or alive during her near-death experience? Unfortunately, no. Even if all medical tests certify her death, we would still have to wait to see if life was restored [emphasis mine] (Sabom, "Light" 49).
Of course, the issue of whether Pam was "really" dead within standstill is an extraordinarily misleading red herring in this context. And it is blatantly irresponsible for Sabom to explicitly state that her NDE occurred "while in this state." As Sabom's own account reveals, her standstill condition had absolutely nothing to do with the time when we know that her near-death OBE began: A full two hours and five minutes before the medical staff even began to cool her blood, during perfectly normal body temperature![19] (Again, see Figure 1.)
Unlike the other elements of her NDE, we can precisely time when Pam's OBE began because she didaccurately describe an operating room conversation. Namely, she accurately recalled comments made by her cardiothoracic surgeon, Dr. Murray, about her "veins and arteries being very small" (Pam's words) (Sabom, "Light" 42). Two operative reports allow us to time this observation. First, in the head surgeon's report, Dr. Robert Spetzler noted that when he was cutting open Pam's skull, "Dr. Murray performed bilateral femoral cut-downs for cannulation for cardiac bypass" (185). So at about the same time that Dr. Spetzler was opening Pam's skull, Dr. Murray began accessing Pam's blood vessels so that they could be hooked up to the bypass machine which would cool her blood and ultimately bring her to standstill. Second, Dr. Murray's operative report noted that "the right common femoral artery was quite small" and thus could not be hooked up to the bypass machine. Consequently, Murray's report continues, "bilateral groin cannulation would be necessary: This was discussed with Neurosurgery, as it would affect angio access postoperatively for arteriography" (185). And although Pam's mother was given a copy of the head surgeon's operative report (which she said Pam did not read), the report didnot say anything about any of Pam's arteries being too small (Sabom, "Shadow" 7).
Many have argued that Pam's accurate recall of an operating room conversation is strong evidence that she really did leave her body during the procedure. But there is at least one peculiar fact about Pam's recollections—in addition to the timing of her experience—which makes a physiological explanation of her OBE much more likely.
General anesthesia is the result of administering a trio of types of drugs: sedatives, to induce sleep or prevent memory formation; muscle relaxants, to ensure full-body paralysis; and painkillers. Inadequate sedation alone results in anesthesia awareness. Additionally, if insufficient concentrations of muscle relaxants are administered, a patient will be able to move; and if an inadequate amount of painkillers are administered, a patient will be able to feel pain (Woerlee, "Anaesthesiologist" 16). During a typical surgical procedure, an anesthesiologist must regularly administer this trio of drugs throughout the operation. But just prior to standstill, anesthetic drugs are no longer administered, as deep hypothermia is sufficient to maintain unconsciousness. The effects of any remaining anesthetics wear off during the warming of blood following standstill (G. Woerlee, personal communication, November 8, 2005).
About one or two in a thousand patients undergoing general anesthesia report some form of anesthesia awareness. That represents between 20,000 and 40,000 patients a year within the United States alone. A full 48% of these patients report auditory recollections postoperatively, while only 28% report feeling pain during the experience (JCAHO 10). Moreover, "higher incidences of awareness have been reported for caesarean section (0.4%), cardiac surgery (1.5%), and surgical treatment for trauma (11-43%)" (Bünning and Blanke 343). Such instances must at least give us pause about attributing Pam's intraoperative recollections to some form of out-of-body paranormal perception. Moreover, for decades sedative anesthetics such as nitrous oxide have been known to trigger OBEs.
Sometime after 7:15 AM that August morning, general anesthesia was administered to Pam Reynolds. Subsequently, her arms and legs were tied down to the operating table, her eyes were lubricated and taped shut, and she was instrumented in various other ways (Sabom, "Light" 38). A standard EEG was used to record activity in her cerebral cortex, while small earphones continuously played clicks[20] into her ears to invoke auditory evoked potentials (AEPs), a measure of activity in the brain stem (39).
Sabom considers whether conscious or semiconscious auditory perceptions were incorporated into Pam's OBE imagery during a period of anesthesia awareness, but dismisses the possibility all-too-hastily:
Could Pam have heard the intraoperative conversation and then used this to reconstruct an out-of-body experience? At the beginning of the procedure, molded ear speakers were placed in each ear as a test for auditory and brain-stem reflexes. These speakers occlude the ear canals and altogether eliminate the possibility of physical hearing (Sabom, "Light" 184).
But is this last claim really true? Since Sabom merely asserts this (and has an obvious stake in it being true), we have little reason to take him at his word—especially on such a crucial point. What is the basis for his assertion? Does he have any objective evidence that the earphones used to measure AEPs completely cut off sounds from the external environment?
Since Sabom does not back up this claim in Light and Death, I did a little research and discovered that his claim is indeed false. According to the National Institute of Neurological Disorders and Stroke, as a matter of procedure, a patient who is monitored by the very same equipment to detect acoustic neuromas (benign brain tumors) "sits in a soundproof room and wears headphones" (NINDS). But a soundproof room would be unnecessary, of course, if the earphones used to measure AEPs "occlude the ear canals and altogether eliminate the possibility of physical hearing." It is theoretically possible that the earphones used in 1991 made physical hearing impossible, whereas the earphones used today do not. However, it highly unlikely, as it would be far cheaper for medical institutions to continue to invest in the imagined sound-eliminating earphones, rather than soundproofing entire rooms to eliminate external sounds. As Gerald Woerlee points out, "earplugs do not totally exclude all external sounds, they only considerably reduce the intensity of external sounds," as demonstrated by "enormous numbers of people ... listening to loud music played through earplugs, while at the same time able to hear and understand all that happens in their surroundings" (Woerlee, "Pam").
After being prepped for surgery, Pam's head was secured by a clamp. By 8:40 AM, her entire body was draped except for her head (the site of the main procedure) and her groin (where blood vessels would be hooked up to the bypass machine to cool her blood). In the five minutes or so to follow, Dr. Spetzler would open her scalp with a curved blade, fold back her scalp, then begin cutting into her skull with a Midas Rex bone saw (39-41). At this point, about an hour and a half after being anesthetized, Pam's OBE began (185). She reported being awakened by the sound of a natural D, then being "pulled" out of the top of her head by the sound (41).
"But," Sabom asks, "was Pam's visual recollection from her out-of-body experience accurate?" (186). That is indeed the question to ask regarding the veridicality of her report.
Pam reported that during her OBE, she was able to view the operating room from above the head surgeon's shoulder, describing her out-of-body vision as "brighter and more focused and clearer than normal vision" (41). In her report of the experience, she offered three verifiable visual observations. First, she said that "the way they had my head shaved was very peculiar. I expected them to take all of the hair, but they did not." Second, she reported that the bone saw "looked like an electric toothbrush and it had a dent in it, a groove at the top where the saw appeared to go into the handle, but it didn't." Finally, she noted that "the saw had interchangeable blades ... in what looked like a socket wrench case" (41). Subsequently, she only reported auditory observations—hearing the bone saw "crank up" and "being used on something"—but most notably the operating room conversation initiated by Dr. Murray.
Given such vivid 'perceptual capabilities' during her OBE, we would expect there to be no confusion about what Pam saw during the experience. So her visual observations provide an interesting test of the notion that her soul left her body while under general anesthesia during normal body temperature. Let us look at each of these in turn.
First, there is the observation that only part of her head was shaved. Perhaps she could have guessed this at the time of her experience, but there is no need even for this in order to account for the reported observation. Surely Pam would have noticed this soon after awaking from general anesthesia—by seeing her reflection, feeling her hair, or being asked about it by visitors. And she certainly would have known about it, one way or the other, by the time she was released from the hospital. Indeed, if her hair had been shaved presurgery, or at any time prior to her general anesthesia, she would have known about it well before her OBE. And patients undergoing such a risky procedure are standardly given a consent briefing where even the cosmetic effects of surgery are outlined—if not explicitly in a doctor's explanation, then at least incidentally in any photographs, diagrams, or other sources illustrating what the procedure entails. So Pam may have learned (to her surprise) that her head would be only partially shaved in a consent briefing prior to her experience, but 'filed away' and consciously forgot about this information given so many other more pressing concerns on her mind at the time. That would be exactly the sort of mundane, subconscious fact we would expect a person to recall later during an altered state of consciousness.[21] And although we are not given the exact date of the operation, Sabom reports that the procedure took place in August 1991 (38). He later tells us that he interviewed Pam for the first time on November 11, 1994 (186). That leaves over three years between the date of Pam's NDE and Sabom's interview—plenty of time for memory distortions to have played a role in her report of the experience. So there is nothing remarkable about this particular observation.
Second, there is her description of the bone saw. But the very observation that provides the greatest potential for supporting the notion that she actually left her body during her OBE actually tends to count against that hypothesis. As Sabom recounts,
Pam's description of the bone saw having a "groove at the top where the saw appeared to go into the handle" was a bit puzzling.... [T]he end of the bone saw has an overhanging edge that [viewed sideways] looks somewhat like a groove. However, it was not located "where the saw appeared to go into the handle" but at the other end.
Why had this apparent discrepancy arisen in Pam's description? Of course, the first explanation is that she did not "see" the saw at all, but was describing it from her own best guess of what it would look and sound like (187).
Precisely! Except that, of course, Pam didn't need to guess what the bone saw sounded like, since she probably heard it as anesthesia failed. An out-of-body discrepancy within Pam's NDE prima facie implies the operation of normal perception and imagination within an altered state of consciousness. Indeed, this explanation is so straightforward that Sabom considers it before all others. And it is telling that the one visual observation that Pam (almost) could not have known about other than by leaving her body was the very detail that was not accurate.
Let us turn to the report of Pam's final visual observation during her OBE, her comment that the bone saw used "interchangeable blades" placed inside something "like a socket wrench case." This detail was also accurate; however, one need not invoke paranormal perceptual capabilities to explain it. As Woerlee notes,
[S]he knew no-one would use a large chain saw or industrial angle cutter to cut the bones of her skull open.... Pneumatic dental drills with the same shapes, and making similar sounds as the pneumatic saw used to cut her skull open, were in common use during the late 1970s and 1980s. Because she was born in 1956, a generation whose members almost invariably have many fillings, Pam Reynolds almost certainly had fillings or other dental work, and would have been very familiar with the dental drills. So the high frequency sound of the idling, air-driven motor of the pneumatic saw, together with the subsequent sensations of her skull being sawn open, would certainly have aroused imagery of apparatus similar to dental-drills in her mind when she finally recounted her remembered sensations. There is another aspect to her remembered sensations—Pam Reynolds may have seen, or heard of, these things before her operation. All these things indicate how she could give a reasonable description of the pneumatic saw after awakening and recovering the ability to speak (Woerlee, "Anaesthesiologist" 18).
And, predictably enough, the dental drills in question also used interchangeable burs stored in their own socket-wrench-like cases.
During anesthesia awareness, and as far from standstill as a person under general anesthesia can be, Pam could have heard her surroundings, but not seen them, since her eyes were taped shut. And the facts of her case strongly suggest that this is exactly what happened. Information that she could have obtained by hearing was highly accurate; at the same time, information that was unavailable to her through normal vision was the very information which was inaccurate. More precisely, her visual descriptions were only partially accurate: accurate on details she could have plausibly guessed or easily learned about subsequent to her experience, and inaccurate on details that it would be difficult to guess correctly.
In other words, OBE imagery derived from hearing and background knowledge, perhaps coupled with the reconstruction of memory, fully accounts for the most interesting details of Pam Reynolds' NDE report. After awakening from inadequate anesthesia by the sound of the bone saw revving up, her mind generated a plausible image of what the bone saw used during her operation looked like, rendered from her prior knowledge of similar-sounding dental drills. But her best guess about the appearance of the bone saw was inaccurate regarding the features of the bone saw that only true vision could discern: whether there was a true groove in the instrument, and where it was located.
Moreover, the fact that Pam's NDE began during an entirely nonthreatening physiological condition—under general anesthesia at normal body temperature—implies that there was no particular physiological trigger for the experience (such as anoxia/hypoxia). Rather, it appears that her NDE was entirely expectation-driven. Before going into surgery, Pam was fully aware that she would be taken to the brink of death while in the standstill state. Awakening from general anesthesia by the sound of the bone saw appears to have induced a fear response, which in turn caused Pam to dissociate and have a classic NDE. Indeed, this makes sense of her otherwise odd report of being pulled out of the top of her head by the sound of the saw itself.
At least five separate studies (Gabbard, Twemlow, and Jones; Stevenson, Cook, and McClean-Rice; Gabbard and Twemlow; Serdahely, "Variations"; Floyd) have documented cases where fear alone triggered an NDE. As Ian Stevenson, Emily Williams Cook (now Emily Williams Kelly), and Nicholas McClean-Rice conclude, "an important precipitator of the 'near-death experience' is the belief that one is dying—whether or not one is in fact close to death" (Stevenson, Cook, and McClean-Rice 45). They go on to label those (otherwise indistinguishable) NDEs precipitated by fear of death alone "fear-death experiences" (FDEs). Physiologically, such NDEs might be mediated by a fight-or-flight response in the absence of an actual medical crisis. In a case reported by Glen Gabbard and Stuart Twemlow, an NDEr dislodged the pin of a dummy grenade he thought to be a live one, producing a classic NDE similar to the one Pam experienced:
A marine sergeant was instructing a class of young recruits at boot camp. He stood in front of a classroom holding a hand grenade as he explained the mechanism of pulling the pin to detonate the weapon. After commenting on the considerable weight of the grenade, he thought it would be useful for each of the recruits to get a "hands-on" feeling for its actual mass. As the grenade was passed from private to private, one 18-year-old recruit nervously dropped the grenade as it was handed him. Much to his horror, he watched the pin become dislodged as the grenade hit the ground. He knew he only had seconds to act, but he stood frozen, paralyzed with fear. The next thing he knew, he found himself traveling up through the top of his head toward the ceiling as the ground beneath him grew farther and farther away. He effortlessly passed through the ceiling and found himself entering a tunnel with the sound of wind whistling through it. As he approached the end of this lengthy tunnel, he encountered a light that shone with a special brilliance, the likes of which he had never seen before. A figure beckoned to him from the light, and he felt a profound sense of love emanating from the figure. His life flashed before his eyes in what seemed like a split-second. In midst of this transcendent experience, he suddenly realized that grenade had not exploded. He felt immediately "sucked" back into his body (Gabbard and Twemlow 42).
Gabbard and Twemlow conclude that "thinking one is about to die is sufficient to trigger the classical NDE" (42). After comparing experiences that occurred in nonthreatening conditions with those where subjects were actually close to death, they also concluded that no particular elements were "exclusive to near-death situations," but "several features of the experiences were significantly more likely to occur when the individual felt that death was close at hand" [emphasis mine] (42). That expectation alone can trigger NDEs in certain individuals, then, is well-documented.
If Pam had truly been out of body and perceiving, both her auditory and visual sensations should've been accurate; but when it came to details that could not have been guessed or plausibly learned after the fact, only her auditory information was accurate. Moreover, it is significant that as her narrative continues beyond the three visual observations outlined above, the remainder of her reported out-of-body perceptions are exclusively auditory. Finally, it is interesting that Pam reports uncertainly about the identity of the voice she heard when her OBE began: "I believe it was a female voice and that it was Dr. Murray, but I'm not sure" (Sabom, "Light" 42).
These facts strongly imply anesthesia awareness, and tend to count against the idea that Pam's soul left her body during the operation. If her soul had left her body, the fact that her account contains out-of-body discrepancies doesn't make much sense. But it makes perfect sense if she experienced anesthesia awareness, particularly when one looks at which sorts of information that she provided were accurate and which were not. Pam Reynolds did not report anything that she could not have learned about through normal perception, and this is exactly what we would expect if normal perception alone was operating during her OBE. It is little wonder that Fox concludes that "the jury is still very much out over this case" (Fox 210).
I had never heard of denture man.....but heres your link for that
The "denture man NDE" is one of those rare, apparently veridical near death experiences. This is an important NDE because it is veridical, apparently proving the reality of a non-localized consciousness, otherwise known as a soul. Therefore all serious students of the NDE should perform a careful analysis of the evidence to see whether this case truly is proof of a non-localized consciousness. The first English language mention of this case was published in the landmark article by the Dutch cardiologist Pim van Lommel during 2001 in the international medical journal, The Lancet ( see page 2041 in the original 2001 Lancet article by Pim van Lommel ).
Early in 2009 I published a website with the known facts of the case as revealed by a transcript of an extensive interview with the male nurse involved (see Terugkeer 2008), together with an analysis of the case below. The Summer edition of Journal of Near Death Studies contains two articles with an ongoing discussion of this case.
This turned out to be a rather more extensive website than originally planned, so here is an index of links to sections of this website.
Unfortunately, many people do not have access to the Dutch language transcripts upon which this story is based. The first anyone outside The Netherlands learned of this case, was in Pim van Lommel's well known article published in the medical journal, The Lancet ( see page 2041 in the original 2001 Lancet article by Pim van Lommel ).
During a night shift an ambulance brings in a 44 year-old cyanotic, comatose man into the coronary care unit. He had been found about an hour before in a meadow by passers-by. After admission, he receives artificial respiration without intubation, while heart massage and defibrillation are also applied. When we want to intubate the patient, he turns out to have dentures in his mouth. I remove these upper dentures and put them onto the 'crash car'. Meanwhile, we continue extensive CPR. After about an hour and a half the patient has sufficient heart rhythm and blood pressure, but he is still ventilated and intubated, and he is still comatose. He is transferred to the intensive care unit to continue the necessary artificial respiration. Only after more than a week do I meet again with the patient, who is by now back on the cardiac ward. I distribute his medication. The moment he sees me he says: 'Oh, that nurse knows where my dentures are'. I am very surprised. Then he elucidates: 'Yes, you were there when I was brought into hospital and you took my dentures out of my mouth and put them onto that car, it had all these bottles on it and there was this sliding drawer underneath and there you put my teeth.' I was especially amazed because I remembered this happening while the man was in deep coma and in the process of CPR. When I asked further, it appeared the man had seen himself lying in bed, that he had perceived from above how nurses and doctors had been busy with CPR. He was also able to describe correctly and in detail the small room in which he had been resuscitated as well as the appearance of those present like myself. At the time that he observed the situation he had been very much afraid that we would stop CPR and that he would die. And it is true that we had been very negative about the patient's prognosis due to his very poor medical condition when admitted. The patient tells me that he desperately and unsuccessfully tried to make it clear to us that he was still alive and that we should continue CPR. He is deeply impressed by his experience and says he is no longer afraid of death. 4 weeks later he left hospital as a healthy man. ( Lommel 2001 )
This is a wondrous story. But the Lancet article contains no mention of the year in which the events occurred. All we know is that Pim van Lommel was not in any way connected with the case, because at the time he was a cardiologist working in the city of Arnhem. This account is actually far to vague for any serious anaysis. So what are the facts related to this story?
The first account of this story was published during August 1991 by Vincent Meijers in a magazine called "Cordiaal" (see page 11 in Autumn "Terugkeer"). This was the result of an interview with the male nurse (TG) who was head nurse responsible for cardiac resuscitation at the time. On 2 February 1994, Mr. Ap Addink, a co-worker of the Merkawah Foundation conducted the first extensive interview of TG (page 12 in Autumn "Terugkeer"). This latter, or the Vincent Meijers account, were presumably the basis for the story in the subsequent 2001 Lancet article.
During 2008, Titus Rivas conducted another, very detailed interview with TG. An extensive transcript of this interview was published in the 2008, Autumn edition of "Terugkeer" (pages 12-20 Autumn "Terugkeer"). Commentary by TG intended as a supplement to this interview was published in the 2008, Winter edition of "Terugkeer" (page 8 in Winter "Terugkeer"). Copies of the Dutch versions of this interview are difficult to come by outside the Netherlands. Moreover, Dutch is not a language in which many people are fluent. So I made a English language translation of this interview, which was checked for accuracy by the editor of Terugkeer and Titus Rivas, the person who conducted this interview. English readers can read the English language translation of this interview by clicking on this link .
The content of the 2008 interview with TG did not differ from the earlier interviews (pages 12 and 20 in Autumn "Terugkeer"), so we can assume the memory of TG is accurate as to what he remembers. TG saw this man for a short moment one more time after his discharge from the hospital at the outpatient clinic, but did not speak about his experience at the time. Some time afterwards, TG saw a newspaper announcement of the death of this man (see page 12 Autumn "Terugkeer"). Accordingly the experiences reported by the man who underwent the resuscitation, are unconfirmed by cross-examination of the patient concerned, simply because the man died sometime after after discharge from hospital (page 12 Autumn "Terugkeer"). Moreover, no cross-confirmation with any other of the parties concerned was possible, or has been done. All this means that our knowledge of this "denture man NDE" is solely from the memories of TG at the time of the incident, and his memories of what the patient told him when he spoke with the man when he saw him again on the cardiology ward a few days after the succesful resuscitation in 1979.
In other words, the denture-man NDE is an experience remembered by one person, TG from an incident occurring during 1979. This incident made a deep and lasting impression on TG. But the reality of this incident was subsequently never cross-checked or confirmed by other persons. This does not mean the experience did not occur, nor does it diminish the reality of the event.
But we must first discuss an important aspect of the transcript of TG before proceeding any further with this fascinating NDE report. This is the differentiation between verifiable fact versus opinion and inference. Just as any other transcript or witness account, these points must be carefully differentiated and separated. So what are we talking about?
These elements are in no way specific to the transcript of TG. Such elements are to be found in all transcripts of any event related by a witness. This in no way reduces the value of the transcript of TG. His transcript contains his verifiable observations, as well as his opinions and inferences based upon experience and learning. And what do we find in the transcript of TG? For example, TG stated clearly that Mr. B could not have been conscious, for various reasons.
53. Interviewer: Naturally, the insertion of the Mayo-tube occurred, at least so it seems to me, within a context when there was still no evidence of a heart rhythm?
54. TG: Yes, there was none at the time. No heart rhythm.
55. Interviewer: So no blood circulation and therefore also no brain activity.
56. TG: Yes!182. Interviewer: So then it is out of the question that he had enough brain activity at that moment, or residual activity in his senses to have observed everything by hearing.
183. TG: Yes, it is out of the question. No, at that moment I can be 100% sure of that, no rhythm, no circulation, and I cannot imagine that after all that time that there was enough oxygen in his brain to listen, or see, or to interpret what he observed. No.
These statements are inferences and opinions based upon learning and professional experience, but are not based upon verifiable measurements at the time. For example:
These somewhat inconsistent inferences and opinions were very reasonable when one considers the condition of Mr. B as described by TG. Indeed, at the time this event occurred, no one would have imagined that Mr. B was unconscious. So the opinions and conclusions of TG at the time were normal and expected. Subsequently he realized that Mr. B was conscious and aware of his surroundings, finally stating in his commentary that:
The most important thing I learned from this event for the rest of my life is that in cases of unconsciousness, coma, sedation (sleep with the aid of medication), anesthesia, is that I always try to take into account that patients may experience, feel, and hear things around him, in spite of what we as professionals may think. And that therefore great caution should be exercised with anything we say or do in with such a patient. Never assume that a patient who is unconscious / comatose / clinically dead / anesthetized or sedated, can make no observations in whatever form.
This is the important difference between opinion and inference, and that of verifiable fact. Mr. B was conscious during the resuscitation in the hospital. Regardless whether this was consciousness of a soul, or consciousness of the body, he was conscious during this period. That was verified by Mr. B's account of his resuscitation.
All this does not reduce the value of TG's testimony in any way. All nurses and physicians involved with such a resuscitation during 1979, as well as during 2010, would have thought the same.
The first part of the story relates to the discovery of the man and the arrival of the ambulance.

Here are two views of the village of Ooij taken from the Kruisweg (translation "crucifix road"). The story does not tell us whether he was found on one of the fields near these houses, but it gives an idea of the countryside around the village of Ooij. These are the facts of his discovery and transport to the hospital in Nijmegen.

The ambulance then came from the nearby city of Nijmegen, and brought him to the Canisius-Wilhelmina Hospital there where he was resuscitated. How long would this have taken? Below is a clickable road map of the most likely route taken by the ambulance (click on the image to go to Google maps.)
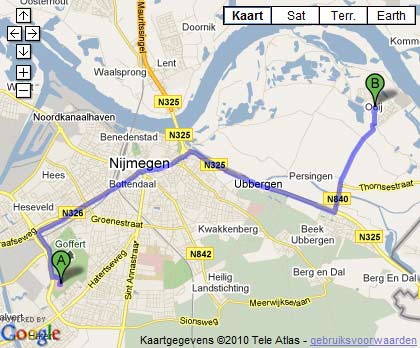
The distance between the village of Ooij and the Canisius-Wilhelmina Hospital is about 12 km (a little more than 7 miles). The ambulance could not have travelled faster on these roads than 80-100 km/hr (50-60 mph). So you have time required to call the ambulance, time to get into the ambulance, time required to drive to the place where the man lay, time to walk-run from ambulance to the man, time to assess the situation. All in all, a total of about 15 minutes at least. This delay between discovery and ambulance resuscitation has several important implications.
Implications of time between falling and arrival of ambulance
The delay between falling, his discovery in the field, and the arrival of the ambulance has far-reaching implications. We know from extensive medical experience, that for people with a normal body temperature, brain damage occurs after 4 minutes of cardiac arrest, and death after 12 minutes (seeMeyer 2000). We know the body temperature of this man at the time of discovery and admission was lower than normal. After all, the ambulance personnel found him lying on the grass in a cold open field, ice-cold to the touch. It is well known that people with low body temperature can survive without any circulation for longer periods than those with normal body temperature. This is the well-known fact that cold meat decays more slowly than warm meat. Total circulatory arrest for 45 minutes is possible at temperatures of 12-14 degrees Celsius (Dobelle 1997, Casthely 1985, Ergin 1982). Increasing body temperature, decreases the time for safe cardiac arrest, so at 16 degrees Celsius safe cardiac arrest time is only 37 minutes (Ti 2003), and it is even less as the temperature rises. So we know from medical fact and experience that he must have had some heart rhythm, otherwise he would have simply have died, or developed severe brain damage while waiting for the ambulance.
This man would have been walking on this field appropriately clothed for the weather, and with a normal body temperature. So when he collapsed, his body temperature would have been normal. Clothing slows body cooling, which is why people wear warm clothing when the weather is cold. So if this man had no heart rhythm pumping blood around his body when he collapsed, he would have developed extensive brain damage and died before his body had a chance to cool. In other words, this man most likely collapsed due to a period of abnormal heart rhythm, but still a heart rhythm that pumped blood around his body. And his clothed body slowly cooled down as he lay there for an undetermined time before discovery.
Resuscitation by the ambulance personnel in the field
The facts relating to the initial resucitation by the ambulance personnel are known.
This brings us to the resuscitatiion in the hospital in Nijnmegen where TG was the head nurse for cardiac resuscitation.
As was intimated by TG, the most likely cause of consciousness was the efficient resuscitation with the Thumper. And indeed, efficient cardiac resuscitation can restore and sustain consciousness (seeConsciousness during Cardiac Resuscitation).
Beekhuizen underwent an OBE during his resuscitation with the following properties and experiences.
Only about 25% of people experience an OBE during an NDE (see Page on OBE's). Furthermore about 7% of persons experience pain during OBE's (see Tiberi-1993 "Extrasomatic Emotions" ). The cause of this is simply that the OBE is an illusion of disembodiment, so that any pain felt is a consequence of the inducing cause of the OBE.
After the successful resuscitation, followed by a week in the intensive care unit, this man recalled the observations made during his resuscitation. He recognized TG immediately from his appearance and/or his unique voice when TG walked inside his room. TG was the man who had removed his dentures! TG was the man who knew where to find his dentures! We read all these things in the transcript.
Now we come to a summary of what has been discussed and determined as medical explanation for the experience of Mr. B.
The only gap remaining in the medical explanation of this OBE/NDE is the question of the timing of the removal of the denture. The transcript reveals some reason to question whether the denture was removed before the Thumper was turned on, or after the Thumper was turned on. However, regardless of this question, one thing is certain, the moment Mr. B arrived at the resuscitation room, adequate resuscitative measures were applied. On arrival of a person in cardiac arrest, people do not stand back, scratch their heads, and start thinking about what they are going to do. Instead they leap upon the person like a pack of wolves and continue resuscitation. If this resuscitation was efficient enough, this would also have resulted in the return of sufficient consciousness so Mr. B would have been able to perceive his dentures being removed. After all, even efficient cardiac resuscitation by hand is sometimes efficient enough to restore consciousness (see: Bihari S, Rajajee V, (2008), Prolonged retention of awareness during cardiopulmonary resuscitation for asystolic cardiac arrest. Neurocritical Care, 9: 382-386.)
So what is left. All aspects of this story have a very adequate medical explanation. Aha, is a commonly heard reaction from the dualists, but a dualist explanation explains this experience just as adequately, and with a lot less complexity. Unfortunately for dualists, oxygen starvation as occurs during cardiac resuscitation also generates OBEs, feelings of transcendence, retention of the ability to hear, etc, etc (many, many human medical studies). So how can the dualist distinguish between an experience due to oxygen starvation in this case, and one which is a manifestation of the soul? It is impossible. This latter consideration renders the dualist position less tenable than that of the materialist.
Finally, the report of "denture man" provides us with unique insights in the genesis of the out-of-body-experience. This fact alone makes it a valuable experience well worth studying. Moreover, this story also gives a clear message - not everyone is unconscious during resuscitation due to a cardiac arrest. But despite the wonderful elements in this story, all elements and observations are explained by the workings of the human body during cardiac arrest and resuscitation. Yet this story is not only a "mere" biological phenomenon, it is also a wonderful demonstration of how the human consciousness may be present during even the most harsh and unlikely conditions.
Cantleave, the evidence you've provided, while certainly worth consideration, does not give any sort of rational explanation as to why these NDEs are occurring. Much of what you've quoted are the writings of militant atheists, such as Dr. Gerry Woerlee (whom I have had several conversations on-line with) who have a much vested interest in going to any lengths to try and explain these experiences away as mere hallucinations. He insists that her experience was caused by anesthesia awareness and will go to any lengths to try and discredit the possibility that our consciousness can survive outside of the physical body. Pam's eyes were taped shut during the surgery, there were nodules placed in her ears that would go off every few seconds and this was used to record any possible brain activity. There's no way she could have possibly either seen what was going on or heard it.
When I compared the descriptions of NDEs with those who have had Anesthesia Awareness, it was pretty obvious that they are 2 completely different experiences. Diane Parr was unfortunate enough to experience AA during surgery and it bares no resemblance at all to those who experience NDEs. People who are blind from birth have been able to see visually for the first time during an NDE, but unfortunately, these experiences too are dismissed by fanatics like Worelee or Susan Blackmore who go to extraordinary lengths to try and discredit them as nothing more than fanciful hallucinations of the brain.
Skeptics (who really are not skeptical at all---they should be renamed: Militant Non-Believers) have long asked for verifiable evidence that something survives the physical death, probably assuming that nothing would ever surface. However, each year, there is more and more evidence that something incredible is going on and it seems to happen as one approaches death. Those who simply have no belief at all in anything but a materialist world will never concede that something might survive the physical death and I find it rather disturbing that so many ex-JWs have simply swapped on set of fanatical beliefs with another and will not admit even the possibility that their view might not be telling the whole story.
I think a good healthy dose of skepticism is something we should all have, but it shouldn't be so fanatical that we're not open to other possibilities. Just because something can't be replicated in a double-blind study under controlled conditions in a lab doesn't mean it's not real.
How can you be so sure and dogmatic about it?
Do you have any evidence the soul or your consciousness DOES NOT continue to live in another world after the physical death?
Let yourself be surprised what happens at your death.
It's not a matter of agreeing with JW's. The Bible view of the soul as the living organism is good science and philosophy.
Aristotle also had a scientific view of the soul compared to Plato.
Resurrection/cloning if there ever were such a thing would not be for your benefit but for the benefit of the community you share.
We really don't have accurate memories of our own histories.
If any of us were cloned we would be up to speed in a jiffy developing enough induced fabricated memory to make people around us happy and after a couple hundred years your current history would dominate and you would hardly care.
Do you care about the 365 days you spent as a five year old?
marked